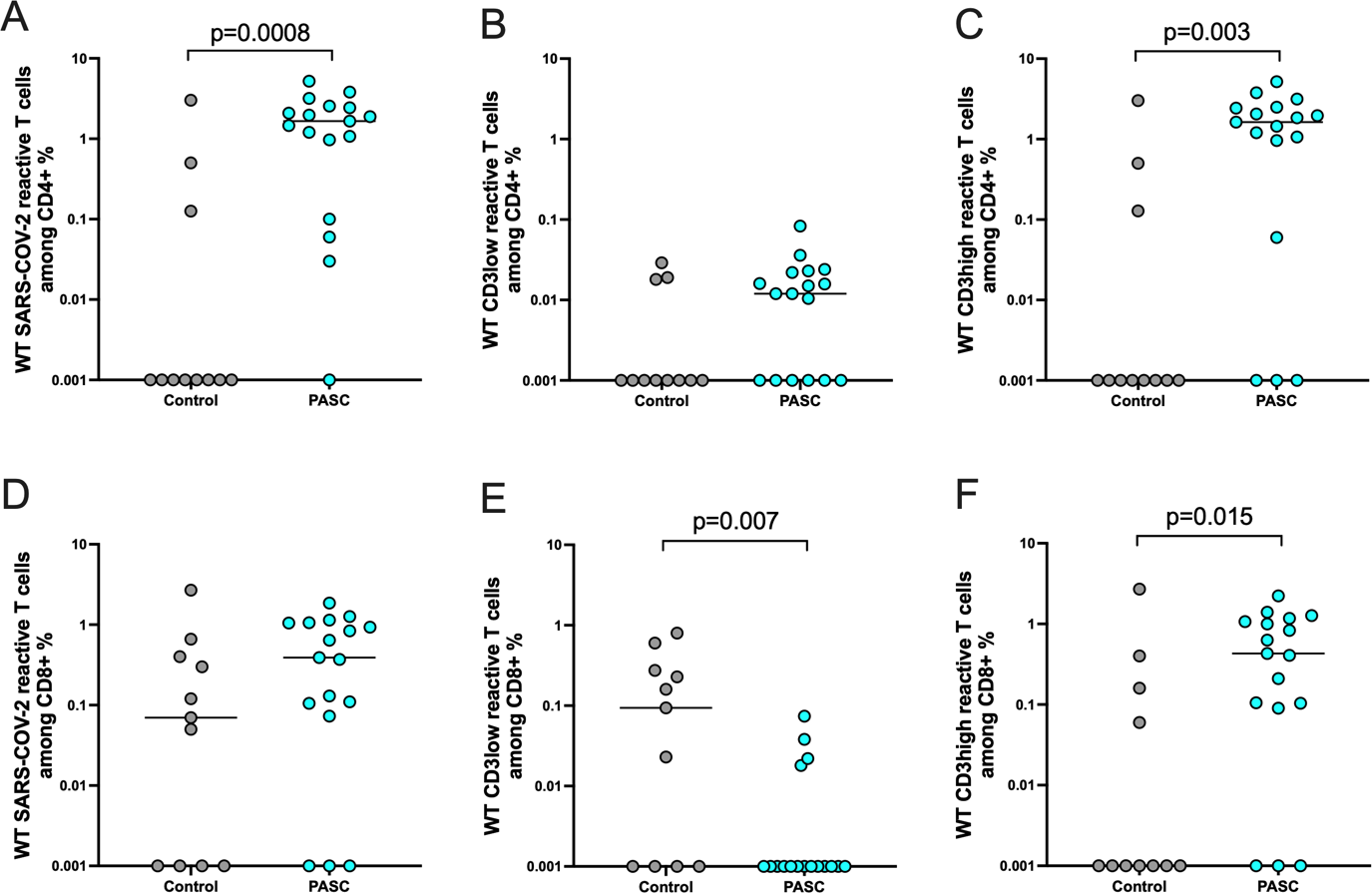
Background: A proportion of the convalescent SARS-CoV-2 pediatric population presents nonspecific symptoms, mental health problems and a reduction in quality of life similar to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and long COVID-19 symptomatic. However, data regarding its clinical manifestation and immune mechanisms are currently scarce. Methods: In this study, we perform a comprehensive clinical and immunological profiling of 17 convalescent COVID-19 children with post-acute COVID-19 sequelae (PASC) manifestation and 13 convalescent children without PASC manifestation. A detailed medical history, blood and instrumental tests and physical examination were obtained from all patients. SARS-CoV-2 reactive T cell response was analyzed via multiparametric flowcytometry and the humoral immunity was addressed via pseudovirus neutralization and ELISA assay. Results: The most common PASC symptoms were shortness of breath/exercise intolerance, paresthesia, smell/taste disturbance, chest pain, dyspnea, headache and lack of concentration. Blood count and clinical chemistry showed no statistical differences among the study groups. We detected higher frequencies of spike (S) reactive CD4+ and CD8+ T cells among the PASC study group, characterized by TNFα and IFNγ production and low functional avidity. CRP levels are positively correlated with IFNγ producing reactive CD8+ T cells. Conclusions: Our data might indicate a possible involvement of a persistent cellular inflammatory response triggered by SARS-CoV-2 in the development of the observed sequelae in pediatric PASC. These results may have implications on future therapeutic and prevention strategies.