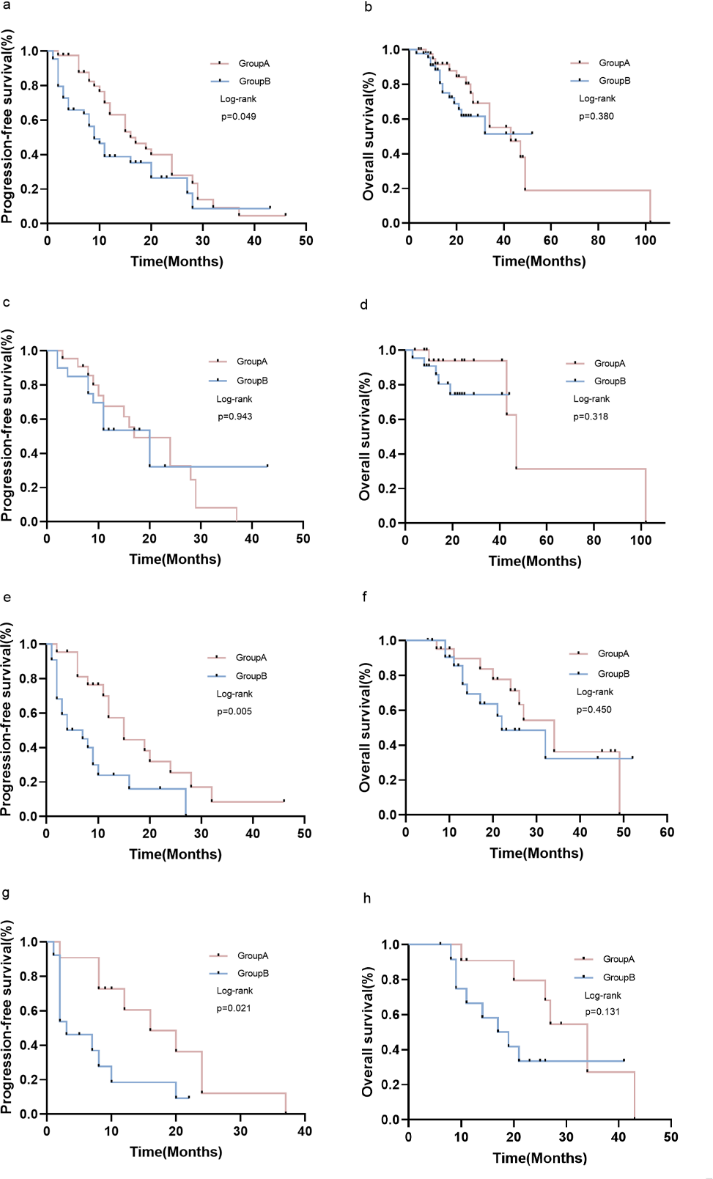
Background: Recently,epidermal growth factor receptor (EGFR) -targeting drugs have benefited thousands of patients with EGFR mutation-positive (EGFR MUT+) non-small-cell lung cancer (NSCLC). Nevertheless, nearly all patients with NSCLC who were sensitive to first- or second-generation EGFR-tyrosine kinase inhibitors (EGFR-TKIs), finally developed resistance. Therefore, numerous clinicians have focused on improving the clinical effect of first-generation EGFR-TKIs (1st-gen EGFR-TKIs). Methods: To analyze the therapeutic outcomes of individuals with progressive NSCLC, a retroactive assessment was performed on 86 patients who were medicated with only icotinib or combined with pemetrexed and platinum-based chemotherapy at The First Affiliated Hospital of Henan University of Science and Technology (HAUST). Results: Eighty-six patients with NSCLC-bearing EGFR-sensitive mutations were retroactively analyzed. The results showed statistical significance in PFS (P = 0.049) and disease control rate DCR (P = 0.031) between icotinib + chemotherapy and icotinib alone, especially in the brain metastases (P = 0.021) and L-858R mutation subgroups (P = 0.05). According to the findings of the multivariate analysis, treatment (P = 0.033) and EGFR mutation status (P = 0.019) were significant predictive variables. The OS comparison between icotinib + chemotherapy and icotinib alone were not significantly different. The study included a total of 1242 patients, of which 648 obtained combined treatment and 594 obtained first-generation EGFR-TKI monotherapy. Analyzing the relevant data from multiple studies, the results showed significant improvements in ORR (RR: 0.63, 95% CI: 0.49–0.82, P = 0.0006), PFS (RR: 0.61, 95% CI: 0.47–0.79, P = 0.0002), and OS (RR: 0.67, 95% CI: 0.51–0.88, P = 0.004) for those on combination therapy. However, there was also an increase in treatment-emergent AEs among these patients. Conclusion: In summary, administering first-generation EGFR-TKI concurrently with chemotherapy provides an edge in the therapeutic management of locally or severely advanced NSCLC that is EGFR-positive. Therefore, EGFR mutation-positive NSCLC (EGFR MUT+ NSCLC) patients in this condition may find it advantageous to consider using 1st-gen EGFR-TKIs in conjunction with chemotherapy (1st-gen EGFR-TKIs + Chemo).